Learn From the Dental Industry's TOP LEADERS!
Sit Chairside withDr. Dennis WellsCreator ofDURAthin® Prepless Veneers- OR -
|
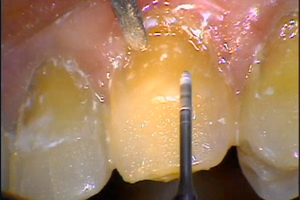
Using Composite Resin in Aesthetic Restorative DentistryPart 1 - Case presentationToday, we're in the office of Dr. Buddy Mopper, here in Glenview, Illinois, a suburb out of downtown Chicago. As you know, Dr. Mopper is the founder of Cosmedent, the leader in restorative products, dental products. And what we have a chance to do today is observe Dr. Mopper perform clinical procedures on two patients. Live procedures, we'll be over the shoulder, and actually see what Dr. Mopper does, that follows his passion, and that is minimally invasive conservative esthetic dentistry. Every one of these restorations should be restored in my mind. The problem with many dental offices is they let these things go. And if you let them go, it will add to the recession aspect of the tooth and you might end up losing gingival tissue. But if you restore these things, will stop the gingival migration of the tissue very easily. It will allow the teeth to have proper brushing habits, it will reduce sensitivity, and it's really one of the ways to get dental practice; you'll not only help the patient, but you'll help yourself financially. There's a lot of restorative aspects of dentistry, they're not being done with composites, and it should be done, and I find it really especially remarkable the restorative materials that we can have and probably dentistry's most versatile material. Now, if you take a look at the right side, you can see that there, that we restored from first molar to canine, and actually the restorations are totally invisible, you can't see them. That's our premise, that we wanna make the restoration so that they disappear in the tooth structure, and it doesn't look like a filling. I don't care what we do with composite resins, but that's the object. And one of the reasons that this is true, is because of the materials that we use. And for cervical restoration, if it's shallow, has no depth, our material of choice is microfill. And the reason of that is because of its tremendous polishing ability. The ability to marginate better than any other material. The ability to stay polished longer than any other material. The best biologic compatibility to the gingival tissue, and the real aspect of total realism that you create because of the refractive, reflective index of this material. And once it's marginated into the tooth surface properly, and that's the whole aspect - you have to know how to handle these materials - it really looks like tooth surface, and it stays that way. The other thing is it has the best flex of all the composite materials. So as the tooth flexes, if the patient does grind a little bit or something like that, this is a material that will stay in the mouth and will not be lost due to any type of clenching or bruxing, better than any other material on the market, and that's why we use microfill. If you take a look at Marcia's left side, and we're gonna work in the upper arch today, she's gonna have some done, also restorative done in the lower arch too, it's part of the old cervical restorations that are there, and new lesions that are there, but if you look at the lateral, the canine, and the bicuspid, those are restorations that we're gonna do today, and it's gonna be a relatively simple procedure, this is really easy to do, if people understand how to do it. These are relatively shallow restorations, and so they will be restored with microfill. If you have to go deeper, and you've got a deeper abfraction, then we will start to bring up the undercover with a nanofill material, because nanofill has more opacity, and then overlay it with a microfill. But in this case, I think we'll probably be able to restore all of them with the microfill material. So this just takes a look at the side that we're gonna be working on today, prior to giving Marcia the injection. We're gonna use the injection using The Wand, which is a very wonderful technique. And it's relatively painless. I always, I always use topical anesthesia before we start. I let it set for about a minute. And then we go ahead and we use The Wand to deliver the anesthesia to the patient. And I always work with anesthesia once we, when we're doing the preparation, because I don't want the patient to move, I don't want them uncomfortable, and if they say to me, “I don't want any anesthesia, I don't need it.” And I'll say, “Okay, but the minute you move, you've got to. Because I can't move, I can't work on a moving target.” So this is what we're gonna do today, are these three cervical restorations. Now what we're gonna do is apply a little topical anesthetic. Let me close it up here. And what that does is it really, really helps because, I've already used topical. You know, I'm a pediatric dentist, that's the way I started. So, if you want to work on a child, the best way to work on them is to not cause any pain. And to work on a patient, any patient, you don't want to cause any pain. The way to make topical work, is make sure that you, it lasts, you leave it on long enough so it has an effect. It penetrates the mucosa really rapidly. And I don't know how many of you use it, but I would strongly recommend it. And then the other technique that we're using, is The Wand. And it's, it's really an automatic technique, and it's a drop by drop technique, and then once we get the penetration, the initial penetration of the anesthesia into the tissue, then we can run it faster. The neat thing about The Wand, is the fact that it's, it's, it's a thrust with a pen grasp. You hold, you hold The Wand in your hand like you're thrusting, holding a pencil, so you have complete control. So I'm gonna place it, and I'm not gonna just drape the lip, and that already starts the injection. She started the head of the needle, so the drop is going in, ahead of the thrust of the needle. And so we do drop by drop . Until I think I've got enough. So we are ready to start. And I run this between 20000 and 40000 RPMs using an electric handpiece usually, to remove this stuff. So we're just gonna remove this. Now, we already took the material out. I'm gonna marginate this. Now, if you'll take everything that I do, that's are we always go beneath the free margin. We'll take this angle along, cutting shape we can do to actually bevel up on the surface with this bur. Because we use, because we use microfill, there's no reason to put in retention. If you wanna put in retention, you can, but we don't. So we don't sacrifice any tooth structure. And our retention rate with cervical restorations are really good. Marcia, are you wearing a night guard? Say yes or no. No. What you really need is to have this canine right and onto this tooth, because you've ground your teeth down so badly that they need to be restored too. That's one of the things that you can do with composite . . . is . . . and maybe that's what we'll do with Marcia if we can talk her into it. If we get the canine rise added back on to the canine so that she's in good disclusion, and she won't have a lot of the problems she's having right now with these abfractions. You can see the wonderful control we have with the electric handpiece. Because it runs at the lowest speed with greater torque, it gives the ability to have more control when you're prepping these teeth. |

 FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement 7/31/2018 to 7/31/2021 Provider ID# 317928
FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement 7/31/2018 to 7/31/2021 Provider ID# 317928
 Submitting...
Submitting...