Learn From the Dental Industry's TOP LEADERS!
Sit Chairside withDr. Dennis WellsCreator ofDURAthin® Prepless Veneers- OR -
|
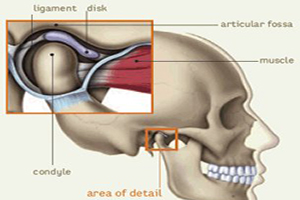
Joint assessment and understanding joint soundsPart 2 - Joint soundsNext brings us to joint sounds. So those are really my two primary palpations that I do as part of my joint exam. Joint sounds is the place where we really need to take our time, go through what we're hearing and think about putting the pieces of the puzzle together. Really for me what I think about joint sounds a couple of things to say is a foundation. One is I don't actually treat joint noise. So when I actually think about moving from the exam and the diagnosis to the treatment options I treat signs and symptoms. So I treat places there is inflammation. I treat patient that are having pain. I don't treat joint noise. Why is that? Because joint noise really tells me it's sort of being to look back in time. The noise tells me about damage that's happened to the condyle disc assembly in the past. It doesn't tell me whether that's actively going on. It could be actively getting worst or it's resolved at this point. But the noise does give me an insight into the history of what's going on in that condyle disc assembly. When I think about joint sounds really there's only one question that I want to answer and that question is where is the disc? So where is that piece of cartilage that's responsible for making sure that that joint is functioning properly? So as I think about answering that question where is the disc really the place to start for me is we have to have understanding of joint anatomy in order to put the pieces together. I have to tell that many many years ago when I first started learning more about this and putting myself through the process of learning, more about treating TMD patients and understanding joint and muscles disorders. I had it in my head that if I just went to enough classes and I studied enough and I learned all of the different presentation that TMD patients will come in with, at some point I'll have them all memorized and somebody would come in and I'll literally be able to look at their history and their exam findings and know exactly what was going on and how to treat them. I know. That was naÔve of me. But really what I've come to understand is I need to be able to understand how all the parts and pieces work together because everyone comes in with a slightly different presentation and I need to puzzle through it for that individual patient. As part of that one of the things that made the biggest difference for me in understanding and making sense of joint sounds and a joint exam was understanding normal TMJ anatomy. And part of the struggle for me was we always look at it into two dimensions. So the picture that you see on the slide is a great two dimensional representation to cross section through the condyle disc assembly, through the TMJ. But yet what's happening and understanding the sounds is really occurring in three dimensions. So getting that picture and I actually heard Peter Dawson say this years ago that once you can visualize in your mind's eye exactly what's happening in three dimensions in the joint you'll be able to make sense of any joint noise or any joint symptoms that a patient presence with. He was so right. Part of it for me was taking a head and neck dissection class again after being out of dental school, spending lots of time working on that concept. But to go through that as a starting point I thought we would do a very rudimentary sort of we called this play arch. You know we're going to do some live theater here today to show you what's going on. So I'm going to be a condyle. And in this particular instance I'm going to be a right condyle. And so my hands claps over my head are going to be the disc. And so we know in normal anatomic situation the disc, that piece of cartilage, sits on top on the head of the condyle. It's actually much thicker on the outer band and has a thin piece of cartilage in the center. So I like to think about it as every once in a while you find a light saver where the center hasn't been punched out completely. It's got that big thick band and then just a little piece on the center. It's actually sitting on top of a condyle. It actually has ligaments that attached on both the posterior and on the medial and lateral. And then of course the lateral pterygoid muscle would be coming out here toward the camera from the front of the disc and the front of the head of the condyle. And so when we have our teeth together, so we're actually intercuspal position, that disc is sitting on top of the head of the condyle. Where is the load? The load is toward the center of our hand or the medial aspect of the head of that condyle. When we first start to open, the first movement we do probably the first 10-20mm of open or here in the US we may said a quarter inch is what called rotation. So the condyle is simply rotating. It's not moving out of the fossa and down the eminence. It's just rotating in the fossa. That load is staying on that medial aspect so toward the center of our head and it just rotates and the disc rotates with it. If we want to continue to open pass that first 20mm or quarter inch, now the condyle disc assembly has to translate down the eminence. So it's actually going to move down the eminence and then when we closed, we're going to un-translate. That's not actually really a word. And then un-rotate until we get back to intercuspal position. As we move from rotation to translation, the load is going to move from the medial aspect further and further out to the lateral. So that by the time we get to the full opening the load is way out here in the lateral aspect of the condyle disc assembly. So in normal anatomy, in normal function the condyle disc assembly is sitting in position with the disc on top of the condyle and as we rotate it stays on top and as we translate it stays on top and then we undo those movements whether that be opening or right or left excursive. Now what we most commonly come across is a patient who has a pop and click in opening. And so one of the ways that the joint can be damage is that little piece cartilage slides forward on the head of the condyle on the lateral aspect or the outside of our head. Now the load when we're in intercuspal positions on the medial the load when we rotate is on medial. So when we have the patient simply rotate we don't hear anything. Now if they have to keep opening they start to translate and we hear pop. That pop is actually the cartilage being squeezed back into the correct anatomic place and after the pop they're underneath the disc and then as they close the disc will slip or slide forward. We don't always hear that second pop or click on closing. Over time from doing this pop every time they open and close that thick outer band of the disc gets compressed and gets thinner so that ultimately between the thinness of the disc and the fact that the load is moving away when we're closing the disc literally can simply slip forward and we don't hear a sound on closing. But if you were hearing a pop on opening translation you can count on the fact that when they close that lateral pole is slipping forward. Other patient will tell us they have a pop or click but then it went away. So on that lateral aspect over time, that piece of disc is getting further forward, getting further damage so when they rotate there's disc between the condyle and the fossa and that's where the load is. They start to translate the disc stays ahead of the condyle and it never comes back into position. Another group of patients will tell us they have a pop or click but actually means the medial pole is off. So the disc is sitting in front of the condyle so that in intercuspal position they're not sitting with disc between the condyle and the fossa. They're actually sitting on and loading retrodiscal tissues. Now as soon as they start to rotate we hear pop. That's that disc getting back into place on the medial pole and then they translate and they're typically off the lateral pole then they go to un-rotate and that disc slides forward. Last group of patients is off on the lateral pole and the medial pole and when they rotate we don't hear a pop or click. We would hear crepitus cause they're on retrodiscal tissue and when they translate the disc stays in front of the head of the condyle. So hopefully that will give you a little visual to put together with when we're about to talk about joint sounds. So when we think about translation. Translation, the load is moving laterally. It's on the lateral aspect and keeps moving laterally through that movement. Translation is the part of the movement that starts after we're already open a quarter inch or 10-20mm and continues all the way through maximum opening. Translation also occurs not just in opening but in right and left excursive and it's what the joint is doing on the balancing side in an excursive movement. So those are translatory movements. Rotation, the load is on the medial aspect to the head of the condyle through the disc. Rotational movements are usually the first 10-20mm or quarter of inch of opening. Just to sort of put this all back together and in right and left excursive movements. Rotation is actually what's happening to the working side condyle. So now when we think about disc displacements and so one of the things I'm going to ask that you think about is when you're writing in a chart, that you not simply put anterior disc displacement because in truth there isn't enough information. That isn't writing down something that is a true diagnosis. I am going to ask you to differentiate. Is it a lateral pole or a medial that displaces and does it get back into position during movement which we call reduction. So if the cartilage disc actually slides back into place, we're going to say it reduces. If it doesn't, we're going to say it doesn't reduce or without reduction. So we think about our joint sound and our disc displacements. A lateral pole with reduction. So what are we going to hear, what is the patient going to tell us? What they're going to tell us is that they have a pop or click when they open or close their mouth. They're typically going to say it happens every time they open their mouth. When we actually palpate their joints or we listen with a Doppler we're going to find that pop or click is occurring during translation. So after they're already open a quarter inch or 10-20mm. Normally when we have what we called a lateral pole disc displacement with reduction where we hear the pop or the click on translation, this is not associated with discomfort. So this is probably the largest majority of the patients who come in and say yeah my joints pop or click when I eat. And there really is no patient complaint of pain. Now what I do here from patients all the time about is they're concerned about the noise. They want to know if the noise is okay. Do we need to do something about the noise and every once in a while I actually have a patient where the noise is so loud and so disconcerting that other people can hear it. And so now there's a whole social implication to the joint noise. But that's a lateral pole disc displacement with reduction. And so, those of you who are familiar with Mark Piper's classifications when we think about this he would call this a three A. It's a lateral pole with reduction. The next one that I'd describe is what we called a lateral pole disc displacement without reduction. So what are we going to hear from the patient? Well what we're going to hear is yup my joint used to pop and click but then they stopped. As we said earlier in this piece they often associate that with now it's gotten better. And so part of it is explaining for them some of the anatomy what's going on. What are going to hear? Well first let's talk about what are you going to feel. Cause probably the most common way that we do a joint exam and we look for a noise is palpable which is putting fingers over the condyle. In a lateral pole without reduction, you aren't going to feel anything because they used to pop and click, that lateral pole that disc does not get back in the right place anymore and very very rare to feel crepitus underneath your fingertips unless it's very course and very far along from a progression standpoint. So you're going to do a joint exam and you're going to go yup they don't have any joint sounds. That's why one of the things we're going to talk about is how important it is to auscultate to actually listen to the joints. So especially if the patient comes in and says I used to pop and click and I don't. We need to know what we're going to hear not just what we're going to feel underneath our fingers. So when we do pick up a Doppler we're going to actually hear crepitus on translation so that kind of crunchy noise. And for those of you not familiar, not using a Doppler, we actually do have a companion piece to this video on the joint exam where we go through using a Doppler to auscultate. What about pain or symptoms. Now this is a situation where I would tell you experientially most patients do not report pain. But there is a small group of patients and I'm actually one of them cause this describes both my right and left joint, lateral pole without reduction where there can be some pain. So how will the patients describe the pain? It's typically a discomfort that they get all the way sort of the extreme ends of their movement so either wide open or all the way out at right and left excursive. Because if you think about the load the load starts on the medial on rotation and moves out laterally in translation. If that little piece of cartilage never gets back in place what they're loading is retrodiscal tissues. In some patient that retrodiscal tissue fibrosis or scars over and its not uncomfortable. And for others because it's highly innovative and highly vascular it stays uncomfortable. It stays inflamed. And so when they're in an extreme position right or left, they may have some discomfort. Now some of those discomforts that patients have in those movements can also be coming from muscle. So we're going to talk at the end of this piece about a diagnostic test to differentiate joint pain from muscle pain when we talk about pain on movement. So that's our lateral pole without reduction and using Piper classification it would be a Piper 3B for that joint. |
 FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement 7/31/2018 to 7/31/2021 Provider ID# 317928
FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement 7/31/2018 to 7/31/2021 Provider ID# 317928
 Submitting...
Submitting...